By Josh Gray and Maria Monahan
The skin substitute cost explosion of 2022 – 2025 should be behind us. But it continues to hang over the finances of ACOs.
Skin substitutes are expensive wound care products made from human placenta and other biologicals. The cost of some of these products exceeded $21K per square inch; ongoing treatment for a single patient could easily run hundreds of thousands — occasionally over $1 million — per year.
While clinicians using skin substitutes predictably defended their approach, most in the industry felt cost growth was out of control and the use unwarranted.
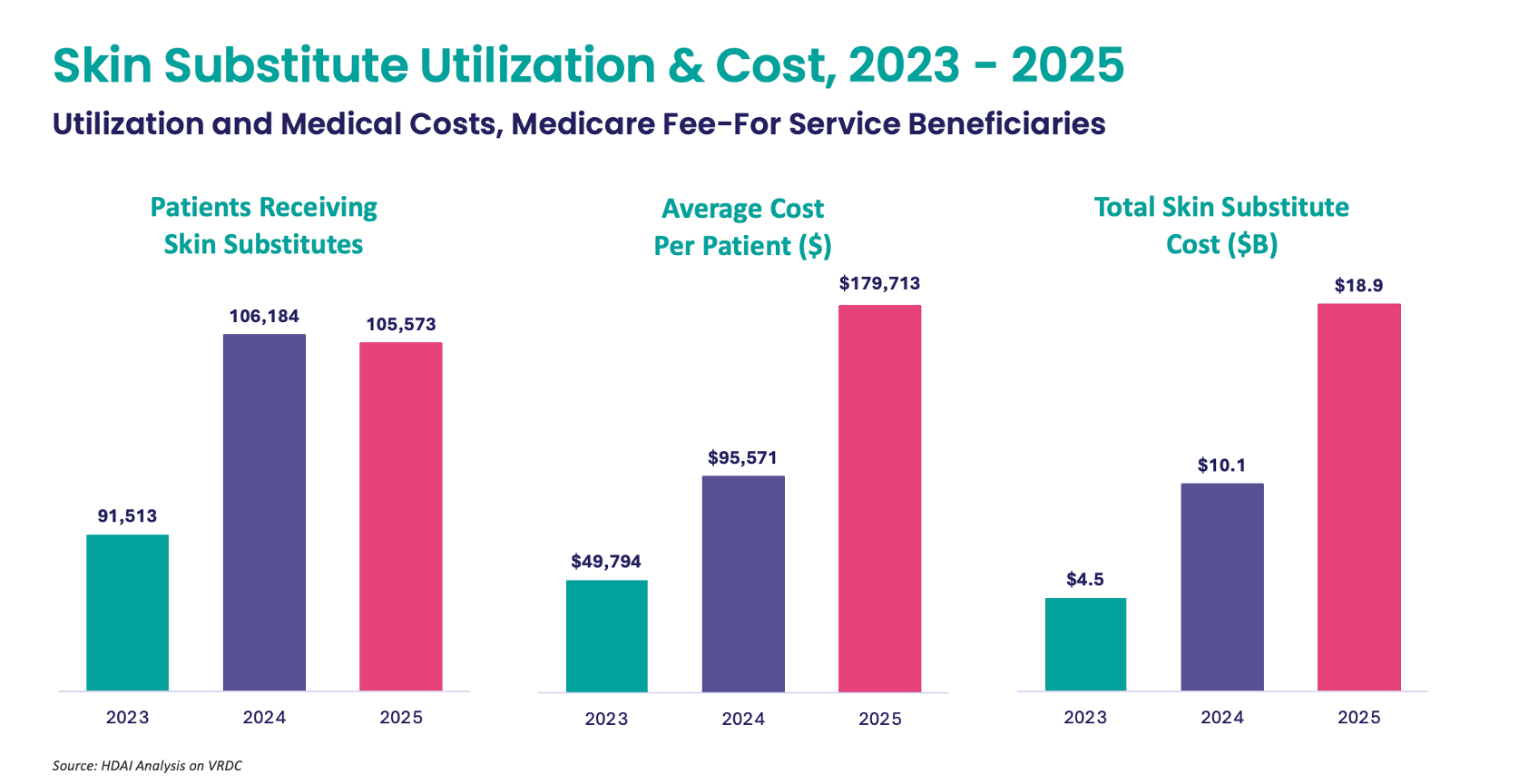
Our analysis of Medicare fee-for-service claims show the explosion of skin substitute expenditures for Medicare patients. Allowed charges increased from $4.4B in 2022 to $18.9B in 2025. Most of this increase was driven by skin substitute cost per patient — which increased fourfold between 2023 and 2025, from $50K to $180K.
Economics drove most of this runaway cost escalation. Through 2025, Medicare reimbursed clinicians providing skin substitute treatment at ASP (average sales price) + 6%, where sales prices for a single square centimeter could run $3K or more. Manufacturers often provided grafts to physicians at steep discounts, allowing them to pocket the difference.
In late 2025, CMS finalized a policy change reclassifying skin substitutes from biological products to incident-to supplies. Previously, these products were reimbursed under the ASP methodology, with each skin substitute assigned its own billing code and payment. Effective 2026 Medicare will pay a flat rate of $127.14/cm², instead of ASP-based payment.
The October 2025 ruling controlled 2026 pricing but left 2025 ACO settlements unresolved until March, when CMS issued a determination.
For High Needs ACOs, the news was positive. CMS acknowledged the disproportionate burden skin substitutes placed on High Needs ACOs (accounting for 12.6% of total program expenses) and agreed to remove 90% of skin substitute expenditures from PY 2025 settlements, recalculate stop-loss and retrospective trend adjustment, and hold ACOs harmless from any downside impact.
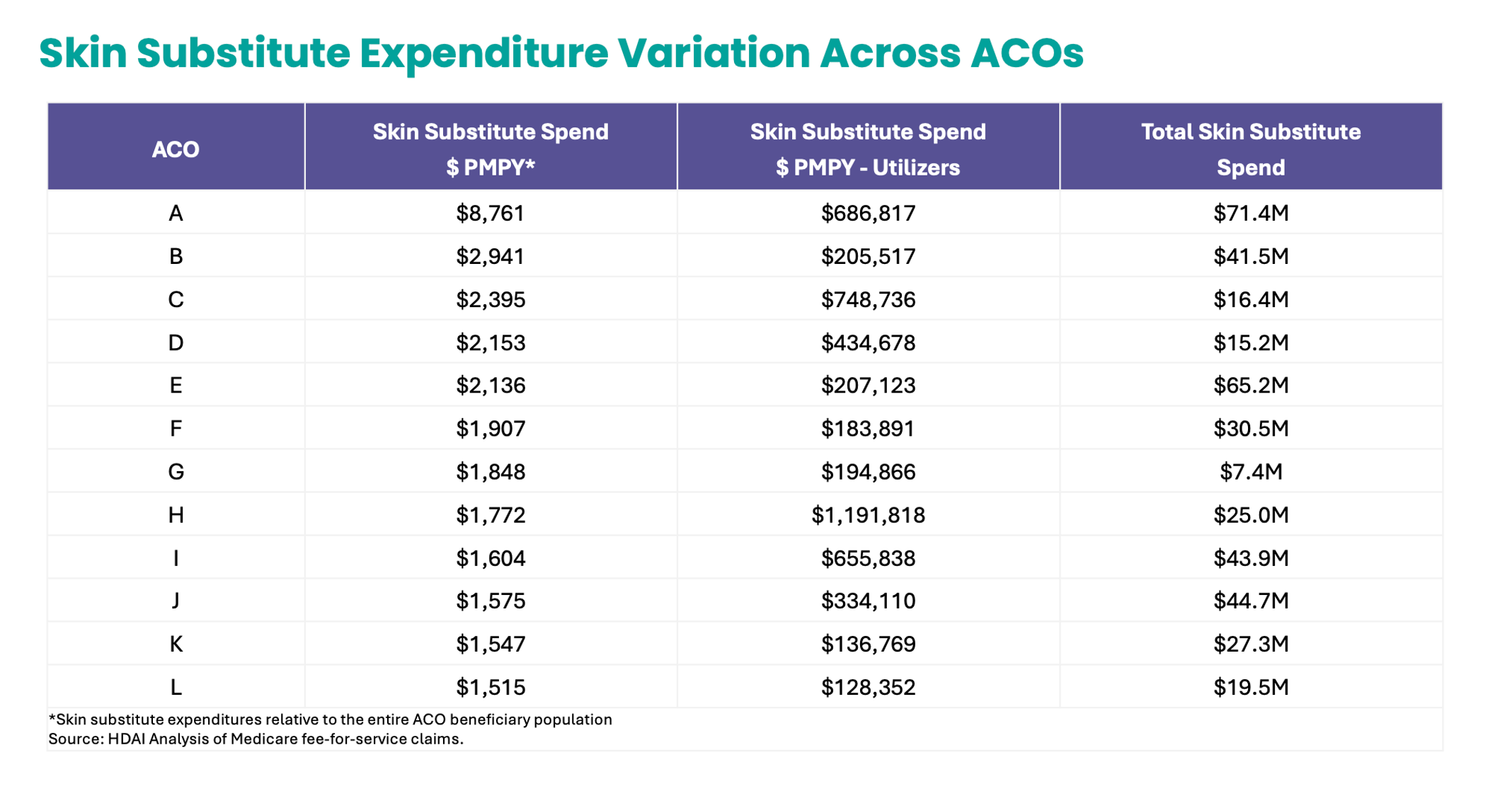
MSSP ACOs were not as fortunate. CMS determined skin substitute costs average less than 2% of total MSSP spending, and that truncation would absorb 65% of costs, leaving 90% of ACOs unharmed. But roughly 48 ACOs still face exposure, disproportionately those serving higher-need populations. We have reproduced the skin substitute burden placed on 12 MSSP ACOs in 2025 below who illustrate the steep financial exposure faced by some.
NAACOS, the AHA, and select ACOs have urged CMS to hold MSSP ACOs harmless for 2025 — a fix CMS should adopt without delay.
Would you like to learn more? Let’s talk.
Josh Gray, VP of Analytic Services, HDAI ([email protected])
Maria Monahan, Data Analyst, HDAI ([email protected])
SHARE