By Josh Gray and Nigel Harriman
The Rural Health Transformation Project is an unprecedented federal initiative that commits $50 billion over five years to reshape healthcare delivery in rural America. Participants are expected to pursue transformative technologies, new care delivery models, workforce innovation, and digitally enabled approaches to care. The scale and scope of this initiative is unprecedented The legislation includes an incentive structure around innovation and accountability. States must submit detailed transformation plans describing how they will improve rural health access, outcomes, workforce capacity, and care delivery. A significant portion of funding is tied to strategy, execution, reporting, and demonstrating progress – rewarding organizations and partnerships that can implement credible, data-driven approaches to improving outcomes and penalizing those who can’t.
In other words, organizations and providers that want to earn and sustain funding will need to show measurable progress against predetermined outcomes. Early in the program, some of these may be process measures, including improving telehealth access or developing workforce trainings and care coordination programs. Over time, expectations will shift toward showing measurable improvement in outcomes, such as avoidable hospitalizations, readmissions, chronic disease burden, total cost of care, or mortality.
Moving clinical outcomes will be a significant challenge. Health outcomes are driven in part by socioeconomics, which vary a great deal across counties and are extremely difficult to influence. Moreover, the health profiles of the 2200 rural counties in the United States vary dramatically. What works in one county may fail in another: to move the dial on outcomes. Providers and public health professionals will need to be surgically focused.
This is illustrated in the graph below, which depicts mortality rates for the roughly 7 million Medicare fee-for-service beneficiaries residing in rural counties in 2025.
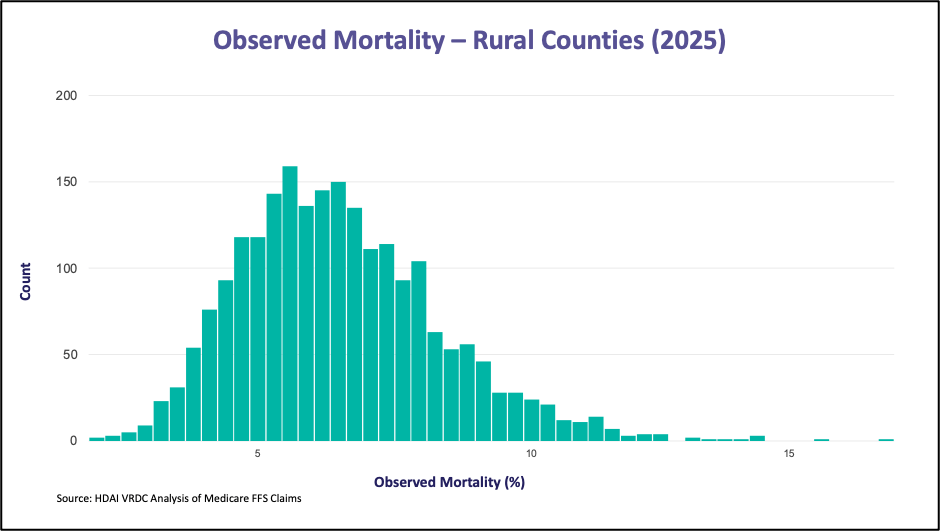
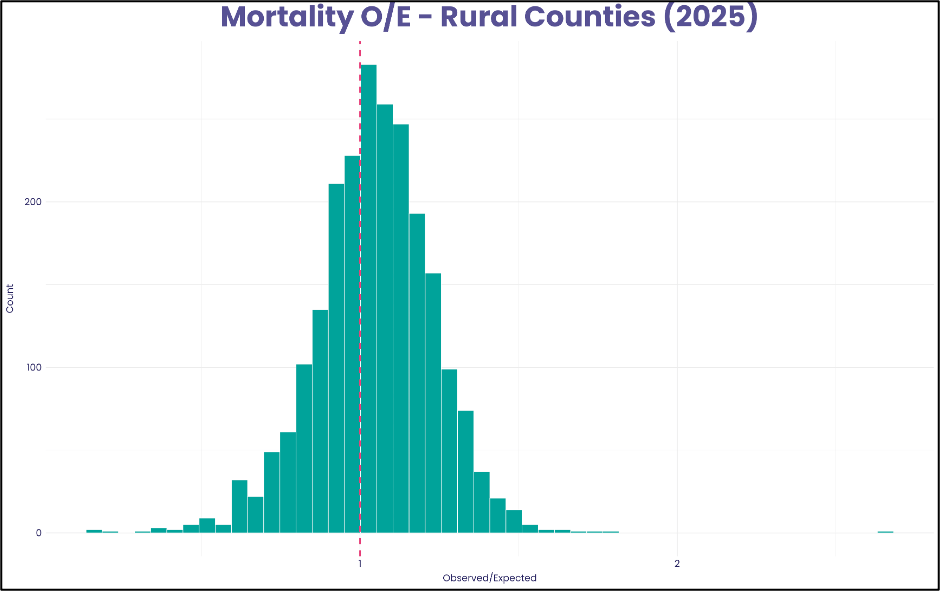
The dispersion is notable: 457 (21%) of counties have mortality rates 25% below the national average, while 403 (18%) have mortality rates 25% above the national average. Importantly, these are unadjusted rates. However, controlling for demographics and medical history explains only part of the observed differences. As shown below, substantial differences remain even after adjustments based on health status and medical conditions, which suggests that local infrastructure, provider access, care delivery models, community conditions, and health behaviors continue to shape outcomes.
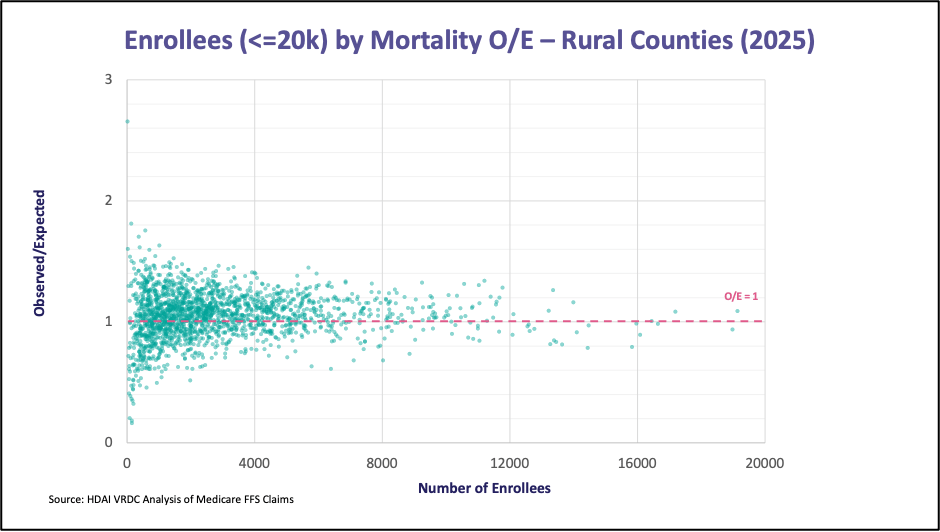
Small rural counties present even greater challenges. As shown below, 23% of rural counties have both higher observed to expected mortality (OE>1) and less than 2,500 people in them. Small rural areas are often further disadvantaged by limited provider capacity, fragile healthcare infrastructure, and insufficient resources to support broad-based transformation efforts.
These observations raise pressing strategic questions for providers and public health leaders. A one-size-fits-all approach will not work – rural counties vary enormously in their demographics, resources, and needs, and will require different types of interventions at and budgets. In many counties, dispersed populations and limited infrastructure mean that remote care technologies will be essential. Interventions that aren’t data-backed and carefully designed to respond to local realities will almost certainly fall short.
If you work with a provider organization or public health entity and are curious about recent outcomes, including mortality, readmissions, ED utilization, or other measures, in your county or counties, please reach out. We would be happy to review relevant data with you.
Josh Gray, VP of Analytic Services, HDAI ([email protected])
Nigel Harriman, Sr. Data Analyst, HDAI ([email protected])
SHARE